What Are the 5 Types of Myocardial Infarction?
The universal definition of myocardial infarction classifies these cardiac events into five distinct types, each with different causes, mechanisms, and treatment approaches.
Below, our specialists in advanced cardiac diagnostics at CardioCare will break down the five types of myocardial infarction so you can better understand this life-threatening condition.
What Is a Myocardial Infarction?
In simple terms, a myocardial infarction is a heart attack. It happens when part of the heart muscle dies because it doesn’t get enough blood. This lack of blood flow, or ischemia, is usually caused by a blocked coronary artery.
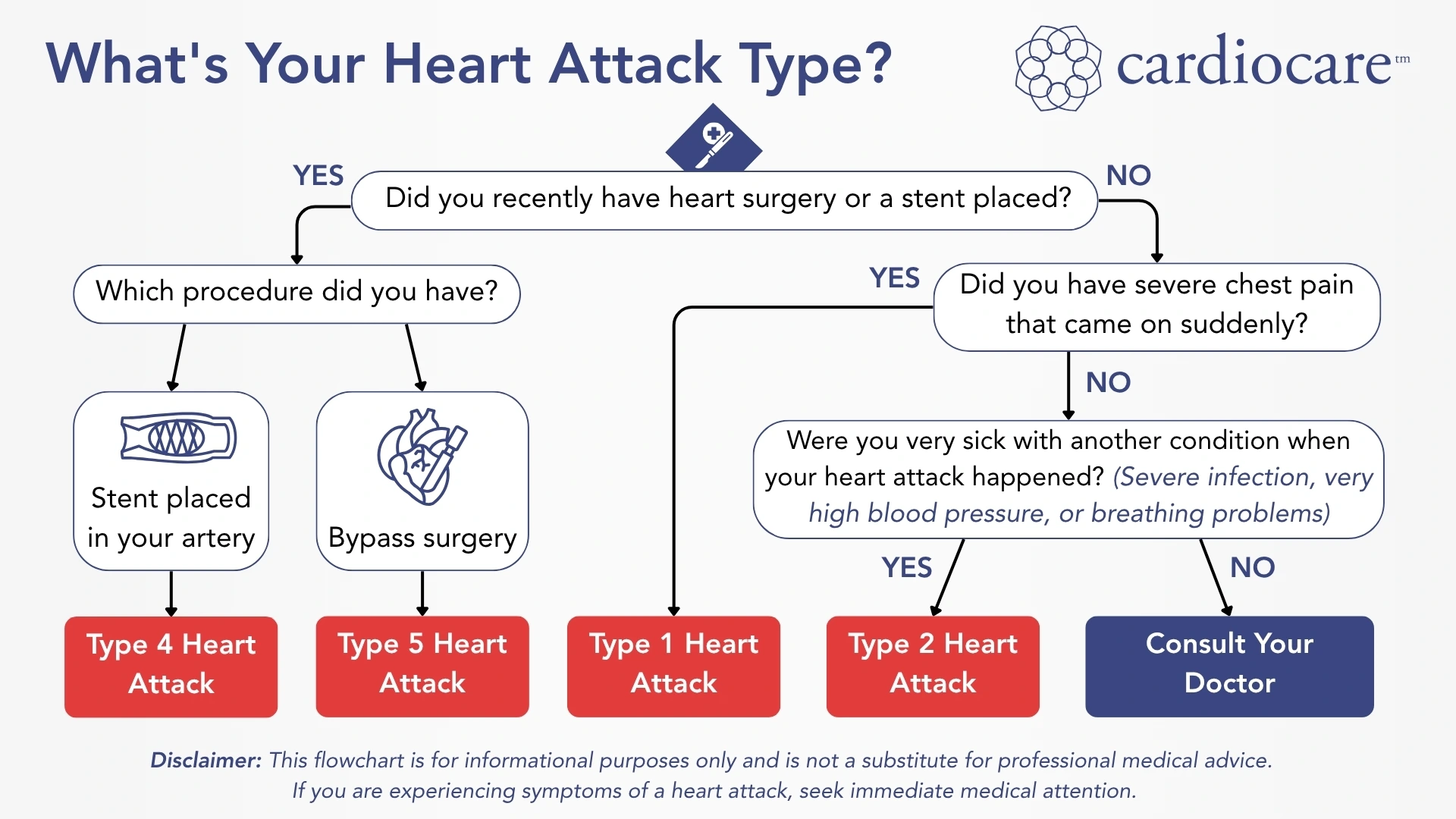
| Type of MI | Primary Cause | Key Characteristics & Context |
|---|---|---|
| Type 1 | Plaque rupture & clot formation | An atherosclerotic plaque ruptures, causing a blood clot that fully or partially blocks a coronary artery. This is the “classic” heart attack. |
| Type 2 | Supply & demand imbalance | Occurs when the heart’s oxygen needs exceed its supply, but without an acute plaque rupture. This can be triggered by conditions like severe anemia, very high blood pressure, or a rapid heart rhythm. |
| Type 3 | Sudden cardiac death | A classification for a suspected heart attack that results in death before a diagnosis can be confirmed. The diagnosis is based on clinical symptoms and often confirmed post-mortem. |
| Type 4 | PCI-related | A myocardial infarction that occurs specifically during or after a percutaneous coronary intervention (PCI), such as angioplasty and stenting. It’s often due to complications such as a clot forming in the new stent. |
| Type 5 | CABG-related | An MI that occurs during or after coronary artery bypass graft (CABG) surgery. This can be caused by surgical trauma, a problem with the new graft, or an existing coronary artery being blocked during the procedure. |
Doctors diagnose a heart attack based on two main things:
- Clinical signs: Symptoms that suggest a heart attack, such as chest pain, shortness of breath, and a squeezing sensation in the chest.
- Evidence of heart muscle death: This is confirmed by blood work. The key test measures levels of a protein called cardiac troponin. If troponin levels are above the 99th percentile, it indicates that heart muscle cells have died, confirming a heart attack.
Type 1 Myocardial Infarction: The Classic Heart Attack
Type 1 myocardial infarction represents the most common form of acute myocardial infarction, though its exact prevalence can vary. This type results from a ruptured plaque or a tear in a coronary artery, leading to a blood clot that forms inside the artery.
Mechanism and Pathophysiology
The underlying mechanism involves a ruptured plaque or erosion with an associated blood clot, creating a sudden blockage of the coronary artery. When atherosclerotic plaque becomes unstable, it can rupture or erode, exposing material that triggers blood cells to clump together and form a clot. This process results in a sudden reduction in coronary blood flow.
The blood clot may be complete or partial, determining the extent of myocardial ischemia and subsequent heart muscle death. In this context, blockage of the original coronary artery typically involves major coronary arteries, significantly reducing myocardial oxygen supply to the affected territory.
Clinical Presentation
Patients with Type 1 myocardial infarction typically present with acute coronary syndrome symptoms, including severe chest pain that may radiate to the left arm, jaw, or back. The pain often lasts more than 20 minutes and may be accompanied by diaphoresis, nausea, vomiting, and shortness of breath.
Types of Type 1 MI
Type 1 myocardial infarction can be further classified based on electrocardiographic findings:
- ST elevation myocardial infarction (STEMI): Characterized by persistent ST-segment elevation on the ECG, indicating a complete blockage of the coronary artery. A STEMI requires immediate treatment to restore blood flow.
- Non-ST elevation myocardial infarction (NSTEMI): Presents without persistent ST elevation but shows other ECG abnormalities such as ST depression or T-wave inversions. This typically involves a partial blockage of the coronary artery.
Treatment Approaches
Emergency angioplasty is a procedure to open blocked arteries. When available within the appropriate time windows, it’s the preferred treatment for ST-elevation myocardial infarction. For patients presenting within 12 hours of symptom onset, immediate coronary angiography and PCI can restore blood flow to the affected coronary artery.
For patients with extensive disease in multiple coronary arteries, bypass surgery may be needed. This is especially the case for those with left main coronary artery involvement or complex coronary anatomy unsuitable for PCI.
Type 2 Myocardial Infarction: Supply and Demand Mismatch

Type 2 myocardial infarction results from an imbalance between the oxygen the heart needs and the oxygen it receives, without a sudden blockage from a plaque and a clot. This type comprises approximately 25 percent of all myocardial infarctions and is more common in older patients with multiple comorbidities.
Causes and Mechanisms
Type 2 MI can result from various conditions that either decrease myocardial blood flow or increase myocardial oxygen demand:
Decreased oxygen supply:
- Coronary artery spasm
- Malfunction of the inner lining of the coronary artery
- Severe anemia
- Hypotension or cardiogenic shock
- Coronary embolism
- Spontaneous coronary artery dissection
- Respiratory failure with severely low oxygen levels in the blood
- Malfunction of the heart’s smallest blood vessels
Increased oxygen demand:
- Severe hypertension
- Sustained, rapid, or irregular heart rhythms
- Increased oxygen demand from hyperthyroidism
- Severe left ventricular hypertrophy
Diagnostic Considerations
Diagnosing Type 2 myocardial infarction requires careful clinical assessment to identify the underlying condition causing the supply-demand mismatch. Cardiac biomarker values, preferably cardiac troponin, will be elevated, but coronary angiography may show stable coronary artery disease (where plaques are present but not actively rupturing) or even normal coronary arteries.
Patients suspected of Type 2 MI often have underlying stable coronary artery disease that becomes clinically apparent during periods of physiological stress. The presence of obstructive coronary artery disease doesn’t exclude Type 2 MI if the clinical context suggests a supply-demand mismatch instead of an acute plaque rupture.
Management Strategies
Treatment for Type 2 MI focuses on addressing the underlying cause of the oxygen supply-demand imbalance. This may include:
- High blood pressure management with antihypertensive medications
- Treatment of arrhythmias
- Correction of anemia
- Management of respiratory failure
- Addressing thyroid disorders
- Optimizing treatment of comorbid conditions
Unlike Type 1 MI, emergency treatment to restore blood flow with PCI or thrombolytics is typically not beneficial for Type 2 myocardial infarction. It may be beneficial, however, if there’s evidence of acute coronary artery occlusion.
Type 3 Myocardial Infarction: Sudden Cardiac Death

Type 3 myocardial infarction describes sudden, unexpected cardiac death where symptoms suggest MI, but death occurs before blood samples can be taken for cardiac biomarker testing. This classification applies when biomarker evidence is unavailable due to the timing of death.
Clinical Context
Type 3 MI is diagnosed when sudden unexpected cardiac death occurs with symptoms suggesting myocardial ischemia, potentially accompanied by new changes on the ECG suggesting a lack of blood flow or evidence of a new blood clot in a coronary artery. This may be identified through findings from an autopsy or a post-mortem angiogram.
To receive this diagnosis, the cardiac biomarkers (troponins) must be unavailable or obtained before their expected rise in the circulation. This type emphasizes the importance of considering myocardial infarction in cases of sudden cardiac death, even without biochemical confirmation.
Type 4 Myocardial Infarction: PCI-Related
Type 4 myocardial infarction encompasses MI related to a procedure to open blocked arteries (PCI) and is subdivided into three categories:
Type 4a: PCI-Related MI
Type 4a is a myocardial infarction associated with percutaneous coronary intervention. The criteria require cardiac troponin elevation greater than 5 times the 99th percentile upper reference limit in patients with normal baseline values.
Diagnostic criteria:
- Elevated cardiac biomarkers (>5x upper reference limit).
- Evidence of myocardial ischemia through symptoms, ECG changes, or imaging.
- Procedural complications such as coronary artery dissection, side branch occlusion, or slow/no-flow phenomenon.
Type 4b: Stent Thrombosis
This subtype involves myocardial infarction due to a blood clot forming inside the stent that a coronary angiography or autopsy confirms. A blood clot forming inside a stent represents a serious complication that can occur acutely (within 24 hours), subacutely (1-30 days), or late (>30 days) after stent implantation.
Risk factors for a blood clot forming inside the stent include:
- Premature discontinuation of dual antiplatelet therapy
- Suboptimal stent deployment
- Underlying prothrombotic conditions
- Drug resistance to antiplatelet medications
Type 4c: Restenosis-Related MI
Type 4c involves myocardial infarction associated with re-narrowing of the artery, typically occurring months after initial PCI. This can result from new tissue growth or new plaque buildup within coronary segments that were previously treated.
Type 5 Myocardial Infarction: CABG-Related
Type 5 myocardial infarction occurs in association with coronary artery bypass grafting. The definition requires cardiac biomarker elevation greater than 10 times the 99th percentile upper reference limit in patients with normal baseline cardiac troponin values.
Mechanisms and Causes
Bypass surgery can cause myocardial injury through several mechanisms:
- Direct myocardial trauma during surgery
- Low blood pressure during or after surgery
- Air embolism, or a tiny particle blocking a blood vessel
- Coronary artery bypass graft occlusion
- Blockage of the original coronary artery during surgery
- Insufficient protection of the heart muscle during cardiopulmonary bypass
Diagnostic Requirements
In addition to elevated cardiac biomarkers, Type 5 MI requires evidence of:
- New pathological Q waves or new left bundle branch block
- Angiographic evidence of new graft occlusion or native coronary artery occlusion
- Imaging evidence of new loss of viable myocardium or regional wall motion abnormality
Clinical Significance
Perioperative myocardial infarction after coronary artery bypass surgery is linked to increased short-term and long-term mortality. Recognizing it early allows for prompt intervention and optimization of postoperative care.
Risk Factors and Prevention
Identifying and managing risk factors is vital in preventing myocardial infarction across all five types. Both modifiable and non-modifiable factors contribute to cardiovascular risk, so prevention strategies are essential for reducing the incidence of acute coronary syndromes.
Modifiable Risk Factors
Hypertension is one of the most significant controllable risk factors, with elevated systolic blood pressure directly contributing to coronary artery disease progression. Managing blood pressure properly can substantially reduce the risk of MI.
Non-Modifiable Risk Factors
Age and gender significantly influence myocardial infarction risk, with men experiencing higher rates at younger ages. Family history of cardiovascular disease and genetic predisposition also contribute to the overall risk.
Lifestyle Prevention Strategies
Regular physical activity strengthens the cardiovascular system and improves overall heart health. A heart-healthy diet rich in fruits, vegetables, and whole grains provides essential nutrients while reducing harmful cholesterol levels.
Medical Prevention Approaches
Cholesterol management with statins effectively reduces the formation of atherosclerotic plaque. Managing diabetes and antiplatelet therapy in high-risk patients suspected of coronary artery disease further decreases the likelihood of future cardiac events.
Diagnostic Approach
Diagnosing a myocardial infarction is a multi-step process that combines clinical evaluation with specific tests to confirm the condition and determine the best course of action.
Cardiac Biomarkers
High-sensitivity cardiac troponin is the preferred biomarker for diagnosing myocardial infarction, providing better diagnostic accuracy compared to traditional cardiac enzymes. The test requires demonstration of a rise and/or fall in troponin values, with at least one measurement above the 99th percentile upper reference limit.
When possible, normal baseline values should be established to detect dynamic changes. Blood samples are typically drawn at presentation and 3-6 hours later to document the characteristic rise and fall pattern of cardiac biomarkers.
Electrocardiographic Findings
ECG changes vary depending on the type and location of myocardial infarction:
- ST elevation: Indicates acute transmural ischemia, typically seen in Type 1 STEMI.
- ST depression: May indicate non-transmural ischemia or reciprocal changes.
- T-wave inversions: Can represent acute ischemia or previous myocardial injury.
- Q waves: Develop over time and indicate established myocardial necrosis.
- Left bundle branch block: May indicate extensive anterior wall involvement.
Advanced Imaging
Coronary angiography continues to be the definitive test for evaluating coronary artery disease and determining appropriate treatment strategies. This procedure can identify:
- Location and severity of coronary stenoses
- Presence of coronary thrombosis
- Coronary artery dissection
- Assessment of coronary blood flow (TIMI flow grades)
Echocardiography can assess:
- Left ventricular function
- Regional wall motion abnormalities
- Mechanical complications
- Impaired myocardial perfusion
At CardioCare, these imaging techniques are used to provide precise diagnostics and guide treatment strategies.
Special Populations & Considerations
While the general diagnostic approach is consistent, certain patient groups may have different symptoms or have unique risk factors that require special consideration.
- Women: Women may experience “atypical” symptoms more often than men, such as nausea, jaw pain, fatigue, and shortness of breath without classic chest pain. They are also more prone to a different type of heart attack (Type 2) and microvascular dysfunction.
- Elderly patients: Older adults can also have atypical symptoms and are more likely to develop complications like heart failure and multi-organ dysfunction.
- Patients with diabetes: Diabetes increases cardiovascular risk significantly. These patients may experience “silent ischemia” (a lack of symptoms) and have accelerated atherosclerosis and higher rates of multi-vessel disease.
CardioCare’s Ongoing Commitment to Excellence in Cardiac Care
The five types of myocardial infarction represent distinct clinical entities needing different diagnostic and therapeutic approaches. Type 1 MI, caused by plaque rupture and thrombosis, typically requires emergency reperfusion therapy. Type 2 MI results from a supply-demand mismatch and requires identification and treatment of underlying conditions. Types 3, 4, and 5 represent specialized circumstances related to sudden death or procedural complications.
At CardioCare, our experienced team of cardiologists provides comprehensive evaluation and treatment for all types of myocardial infarction. Since 2007, our forward-thinking cardiologists have been working with patients to provide excellent hands-on care. Contact us today to learn more about our advanced cardiac care services and how we can help protect your heart health.
LOCATIONS
Contact us for more information.